Received: Thu 10, Jul 2025
Accepted: Fri 25, Jul 2025
Abstract
Importance: When should we amputate a chronic diabetic foot osteomyelitis (DFO) and when treat it conservatively?
Objective: We conduct a narrative, literature review and develop a questionnaire soliciting the opinions of (inter)-national DFO experts.
Evidence Review: In selected cases, the surgical and and the conservative, medical options yield similar treatment success rates of approximatively 60% to 75%.
Findings: In detail, a direct surgical approach should be reserved for recurrent DFO episodes at the same localization, probably for sesamoid and calcaneal osteitis, extended bone destruction beyond just cortical lysis, progressive local ischemia, and extensive skin breakdowns not amenable to primary wound closure.
Conclusions and Relevance: By identifying these exceptions, surgeons may spare time and resources instead of passing through an (unsuccessful) conservative approach to DFO.
Keywords
Diabetic foot osteomyelitis, surgical resection, amputation, conservative antibiotic treatment, clinical decision
1. Introduction
The optimal therapeutic first-line approach for diabetic foot osteomyelitis (DFO) is one of the most debated issues when treating foot complications in persons with diabetes mellitus [1, 2]. In the last two decades, several research groups have advocated for treating selected DFO cases with antibiotic therapy, with or without only minimal debridement, to halt infection and bone destruction [3, 4]. This approach, often called “conservative”, has typically been used only in patients with uncomplicated DFO [4], especially when infection is limited to the forefoot [5, 6]. Amputations predispose to new ulcerations and infections by shifting weight-bearing mechanics, putting new foot areas under risk [1, 7-9]. The conservative approach (minimal surgery, avoidance of amputation) also has potential problems, including potentially longer duration of antibiotic therapy and no guarantee for definitive success [10, 11]. After initial conservative antibiotic therapy (with minor surgical debridement as needed), those who fail initial may undergo primary minor amputation, or if needed a more major amputation as the salvage strategy [9]. However, the downsides of this sequential approach are the necessity for iterative wound debridement, prolonged need for outpatient visits, increased healthcare costs, the possible selection of (gram-negative) multi-resistant pathogens [12], and a 5%-15% risk for antibiotic-related adverse events [13].
We performed a narrative literature review comparing a first-line antibiotic treatment versus a surgical amputation for DFO. To supplement the published data, we conducted a survey among selected experts, both in Switzerland and internationally. This publication is based on a doctoral thesis, embedded in a quality-of-care project, aimed at streamlining the decision for the first-line approach to DFO, especially among the elderly patients we most frequently treat.
2. Materials and Methods
2.1. Literature Review
I.G., S.F., and I.U. performed an extensive narrative literature review using the MeSH terms “antibiotic", “amputation", “resection”, “conservative”, “diabetic foot osteomyelitis”, or "guidelines" in combinations in German and English languages in PubMed and Google Scholar. They broke down the information into 18 “best-guess" variables frequently encountered in the literature: renal failure; patient comorbidities, limb ischemia, peripheral neuropathy, prior amputation, abscesses, exposed bone, degree of bone destruction, ulcer size/wound grade, gangrene, necrosis, severity soft tissue infection, soft tissue loss, systemic infection/sepsis, drug interactions and side effects of the antibiotic therapy, biomechanical foot deformities, and localization of DFO (Table 1 and Supplementary Appendix 1).
The five most frequently expressed opinions are indicated in bold and underlined.

2.1. Questionnaires
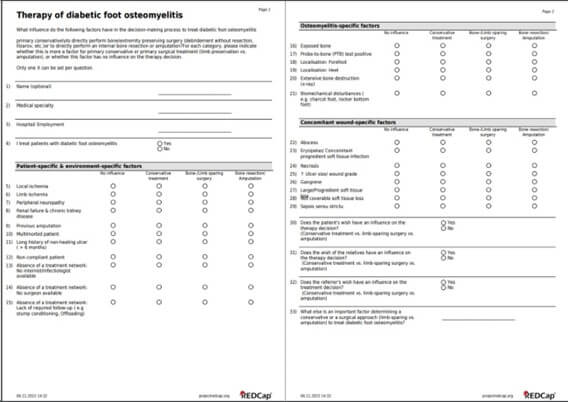
Based on our own experience and literature review, we summarized clinical questions of interest into an online questionnaire based on the REDCap™ (Research Electronic Data Capture) software. We had a German version (for domestic use) and an English version (international use; Figure 1). Before emailing them twice in 2023, we validated them at the Balgrist for comprehensive uncertainties. We chose eighty experts, working in infectious diseases, vascular surgery, diabetology and orthopedic foot surgery, with whom we had some degree of professional and/or academical collaboration in the past. Many were active in writing the 2023 International Guidelines on the Diabetic Foot (IWGDF) [11-13].
2.2. Statistical Analyses
We only used descriptive statistical analyses in this review.
3. Results
3.1. Literature Review
The complete work is an extraction of 118 papers with their own original data and published in the scientific literature (Supplementary Appendix 1). The majority of the scientific literature comes from resource-rich countries in North America (n=39; 33%), Europe (n=67; 57%), or Asia (n=9/118; 8%). These publications frequently employed an international collaboration of authors, in contrast to papers from other regions. We attributed 32 articles to the Mediterranean region (27%) and ten to resource-poor countries. Almost all were published in the 21st century, in surgical (34%) or general medical (65%) (infectiology or endocrinology) journals. The surgical publications mostly originated from Spain (Int J Low Extrem Wounds) or the US (Foot Ankle Surg or Foot Ankle Int), probably because of the preferences of the (inter)-national opinion leaders. The specialization of the journal did not exclude a mixed authorship in the majority of papers. The opinion leader was the last author or was positioned ahead of the last position.
Table 1 shows the ranking of the different clinical parameters in favor of a primarily surgical or a medical approach. Numerically, there were more recommendations for direct amputation than for the conservative approach (Supplementary Appendix 1). While the experts were more in favour of the direct surgical approach than the conservative first-line therapy, the latter almost always remained as an alternative possibility. Frequently cited parameters in favor of a direct surgical approach were: severe ischemia; gangrene; sepsis; major soft tissue loss; and calcaneal DFO [14]. In contrast, many groups preferred a conservative approach for forefoot osteitis without exposed bone. Interestingly, we could not determine the maximal extent of bone destruction (cortical lysis or bone loss, sequestrum) or the extent of skin breakdown to “allow” a conservative treatment. Surprisingly, neither the pathogens (e.g., fungi, multi-resistant microorganisms) nor immune-suppression (beyond the diabetes, e.g. dialysis, alcoholism, transplantation, immune-suppressive drugs) had a decisive role.
3.2. Online Questionnaires via REDCap™
In a second step, we retrieved the professional opinion of 24 experts (via on-line formulary in REDCap™; Figure 1). These included ten active infectious diseases physicians and fourteen orthopedic surgeons, all of whom had long-term clinical and academic experience in DFO management, and with whom we had collaborated in the past. Among eighty experts initially contacted, 21 (26%) responded. We grouped the experts according to those working in Switzerland and those abroad, in order to detect particularities and potential biases. The answers were complete in over 90% of the returns. The experts were congruent with the opinion in the literature (which they had largely written themselves to a great extent).
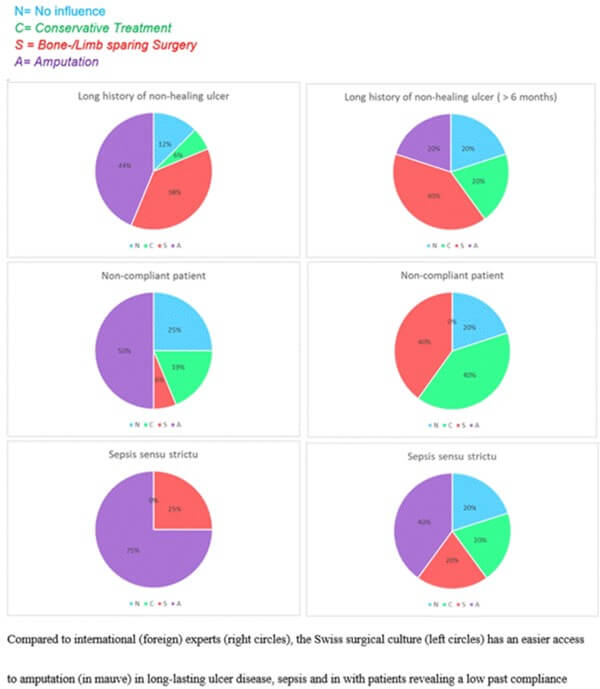
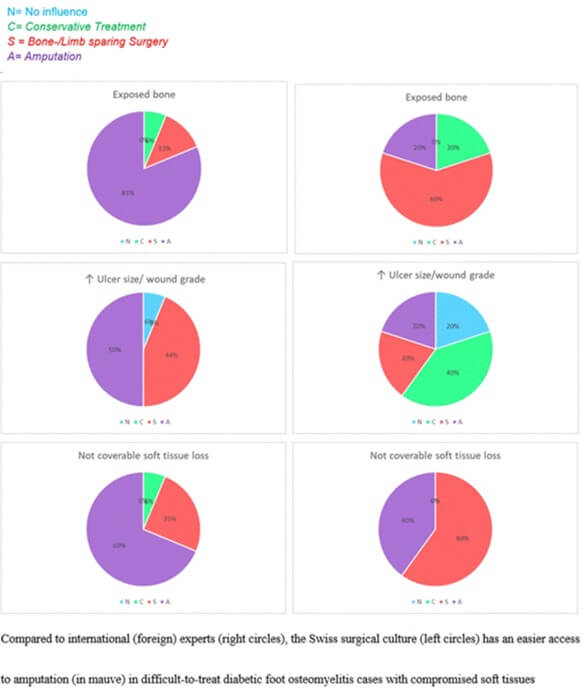
The general consensus was that for forefoot (in contradistinction to hindfoot) DFO, clinicians can attempt a conservative treatment approach. Compared to international experts, Swiss surgeons, all infectious diseases physicians, were less hesitant to amputate in in patients with long-lasting foot ulcers, sepsis, or a past history of poor treatment compliance (Figure 2). Similarly, in Switzerland, DFO cases with major tissue losses, and presumably consecutive difficulties for primary closure, were more likely to have an amputation than patients in other countries (regardless of the type of physician answering the question). In contrast, these soft tissues deficiences played a less important role in decision making for foreign experts (Figure 3), who probably relied more on secondary wound closure.
3.3. Patients’ Wishes
In the opinion of the Swiss physicians, the patient's wish has an important influence on the initial therapeutic decision, with a prevalence of 94%. The wishes of the relatives would influence this decision to 68%. Among the non-Swiss physicians, the specialists state they follow the patient's wishes 100% of the time. The wishes of the patient's relatives and the referring physician also influence the decision, accounting for 80% and 60% respectively. We ignored the impact of patients and families’ preferences after the failure of the first-line approach, as this was not part of our study questions. For health care providers, the failure of a strict first-line conservative approach often led to an ultimate surgical solution.
3.4. Internist Elements of Decision
Frail patients with multiple morbidities “predict” a conservative approach on the part of the Swiss physicians 50% of the time, compared to 80% of international physicians. In Switzerland, the presence of local ischemia (or necrosis) tends to favor a decision for direct resection. In contrast, in the view of non-Swiss experts, the presence of dry ischemia generally predicts a conservative attempt. Advanced peripheral neuropathy has no influence on treatment decisions for either the Swiss or the international physicians (56% vs. 80% in favor of surgery). Renal failure and/or dialysis has no influence on the therapy decision in Switzerland, but international experts are divided fifty-fifty on that matter.
3.5. Surgical Elements of Decision
Previous (toe) amputation has no influence on decisions for treating DFO by Swiss physicians (63%). For international physicians, such a past history would lead to a conservative approach in 80%. In both surveys, the presence of soft tissue abscesses favors a conservative treatment (56% Swiss vs. 60% international). The presence of a cellulitis or erysipela accompanying the DFO does not influence decision (Swiss 31% vs. international 40%) in favor of amputation. In the presence of biomechanical (architectural) disturbances, both the Swiss and international experts recommend limb-preserving surgery or an amputation.
3.6. Differences Among Experts
The most striking differences between the Swiss and international physicians are for sepsis sensu strictu, and the presence of exposed bone. Sepsis frequently triggers a decision for amputation in Switzerland, even if the patient has been stabilized. Foreign experts, especially the ID physicians, are less categoric (Figure 2). In the presence of sepsis, 75% of the international specialists would tend towards a primary amputation, while the remaining 25% would prefer a preserving surgery that is limited to (iterative) debridement of soft tissues. Internationally, 40% would opt for direct amputation in sepsis. However, 20% of international specialists would also prefer a first-line conservative approach in the absence of a rapidly spreading soft tissue infection such as necrotizing fasciitis or (gas) gangrene. Likewise, with a majority of 75%, Swiss specialists prefer primary amputation/bone resection in the presence of a gangrene (infected necrosis). In this situation, international specialists would perform a limb-/bone sparing surgery in 60% of cases, primary amputation/resection for the other 40%.
3.7. Presence of Bone Exposed
In most of the published literature, the presence of exposed bone usually leads to a direct surgical option. International experts are more reluctant. In this study Swiss specialists favour an amputation in 81.25% of such cases, while only 20% of international experts would favor this procedure. Among the international experts, 60% would primarily perform a limb- or bone- sparing surgery. Similarly, among the Swiss physicians, a positive probe-to-bone test facors an amputation in 63% of cases, independent of the extent of bone destruction or lysis. Among the international experts, 40% would prefer the conservative approach when the underlying bone is viable, 20% would tend towards amputation or limb/bone-sparing surgery, while for the remaining 20% this has no influence on the treatment decision. In the presence of a large soft tissue loss (not necessarily with exposed bone), both the Swiss and international experts would opt for direct resection (75% vs. 60%, respectively). Finally, many clinicians suggested they would first address any possible vascular pathologies before (scheduled or non-urgent) surgery. If there was striking improvement after reperfusion, then they would prefer bone sparing surgery.
4. Discussion
DFO is difficult to treat. The final outcomes largely differ based on a variety of patients, wound, and infection specific factors [15]. Its management requires a multidisciplinary approach, with a wide variety of medical, surgical and other healthcare professionals, as well as the patient's compliance with the proposed treatment [1, 8]. The guidelines from the Infectious Disease Society of America (IDSA) [1, 3] and the International Working Group on the Diabetic Foot (IWGDF) [11] provided many evidence-based recommendations on multiple aspects of managing DFO. They cannot, however, give evidence-based in-depth guidance regarding the optimal first-line approach. The updated IWGDF/IDSA 2023 guidelines recommend considering antibiotic treatment without surgery in case of uncomplicated forefoot DFO [11, 12]. However, in case of extensive or ulcers or higher (more severe) wound grades, most of the literature encourages a surgical approach [2, 3, 7, 16-21].
As updated guidelines on this topic have not been issued in Switzerland, we conducted a non-systematic literature review on the most critical points that may help determine whether to select an initial conservative or a surgical approach for DFO. Besides the patient’s preference, the three most influential variables favoring a first-line surgical amputation are: bone at air (exposed); extensive soft tissue loss (that cannot be closed by a flap); and the presence of gangrene (Table 1). The only factor clearly favoring a conservative (avoiding amputation) approach would be DFO limited to the forefoot (toe). Faglia et al. state that “a higher rate of transtibial amputation is found when osteomyelitis involved the heel instead of the midfoot or forefoot in diabetic patients” [22], a view confirmed by other groups [17, 18]. The same approach applies for sesamoid osteitis, which recurs frequently if not surgically resected [19, 20].
Another important aspect in deciding on an initial therapeutic approach to DFO is the presence of peripheral vascular (arterial) disease. If this is present, and successful revascularization is deemed unlikely, many surgeons would refrain from performing an amputation. To add a semi-objective measurement to aid in that decision, many rely on the transcutaneous oxygen pressure measurement. Its predictive value regarding an uneventful wound healing is, however, biased by the effects of many skin/soft tissues conditions, such as edema, and it lacks a strong evidence for predicting clinical success [23]. In the paper by Tone et al. [24] regarding the duration of systemic antibiotic administration for conservative treatment of DFO, patients were excluded if they had an absence of both anterior and posterior pedal pulses by doppler examination. Of note, our interviewed experts did not spontaneously comment on these detailed parameters, and we did not specifically ask them about vascular aspects. Other parameters that may be considered in treating DFO’s, but do generally do not (at least in resource-rich countries) influence the choice between conservative treatment and direct resection, include: the causative pathogens isolated from bone; the antibiotic-resistance of the pathogens; the duration of antibiotic administration; the costs of potentially appropriate antibiotic agents; the size and duration of any underlying ulcer; the degree of peripheral neuropathy; or, various laboratory results [25].
In an editorial published one decade ago, Lipsky [26] proposed factors that favor a primarily conservative (medical) or surgical approach for treating DFO. Favoring conservative: patient is too medically unstable for surgery; poor postoperative mechanics of foot is likely; no other surgical procedures on foot are needed; infection is confined to small, forefoot lesion; no adequately skilled surgeon is available; surgery costs are prohibitive for the patient; patient has strong preference to avoid surgery. Favoring surgical: foot infection is associated with substantial bone necrosis; foot appears to be functionally non-salvageable; patient was already non-ambulatory; patient is at particularly high risk for antibiotic-related problems; infecting pathogen is resistant to available antibiotics; limb has uncorrectable ischemia (precluding systemic antibiotic delivery); patient has strong preference for surgical treatment. These latter recommendations are obviously ID-based, and perfectly encompass the antibiotic aspects, but might not be fully integrated into the surgical clinical mindset. Another review of managing DFO by Lázaro-Martínez et al. [27] in 2019 offered their criteria for favoring either a medical or a surgical approach to treatment. Aragón-Sánchez [20] also stressed the importance of having a surgeon available with sufficient expertise to not only resect the infected bone, but to correct any bone deformity that may have or could cause future foot problems.
Our work has some important limitations. First, it is an opinion survey rather than an analysis of composite original data. Second, we chose a combined classical medical and surgical review as well as a questionnaire design. Third, we assessed the practical opinion of experts practicing in resource-rich countries. Accordingly, the financial aspects, political and resource issues were less relevant when deciding on the best first-line approach. Very likely, the opinions and practices in resource-poorer settings would be more influenced by local reimbursement politics, resource availability, and perhaps by a larger variability in the patient's beliefs and opinions [28]. Finally, we assessed opinions specifically on conservative treatment vs. surgical resection. Hence, we cannot comment on other (intermediary) approaches such as curettage without resection [29], or percutaneous partial bone excision [30].
5. Conclusion
In Switzerland, the patient’s choice (supplemented by those of their family) is a strong determining factor when it comes to decide the initial therapeutic approach in chronic DFO. Based on our literature review and the results of our questionnaire survey we that that we have provide as a minimal consensus that in the absence of a medical emergency in compliant patients, chronic DFO should be treated first-line by targeted antibiotic-based treatment. A direct surgical approach should be reserved for recurrent DFO episodes at the same localization, probably for sesamoid and calcaneal osteitis, extended bone destruction beyond just cortical lysis, progressive local ischemia, and extensive skin breakdowns not amenable to primary wound closure. More international, and preferably prospective, research is necessary to further streamline these multidisciplinary decisions.
Data Availability
Key data are available upon reasonable scientific request to the corresponding author.
Conflicts of Interest
None.
Funding
None.
Acknowledgments
We thank Ms. Corina Früh from the Unit for Clinical and Applied Research (UCAR) at Balgrist University Hospital for her invaluable help.
Author Contributions
Conceptualization: I.G., M.S., F.W.A.W., and I.U. Methodology: I.G. and I.U. Validation: I.G. and I.U. Investigation: I.G., F.S., and I.U. Resources: M.F. and I.U. Data curation: I.G., F.S., M.S., and I.U. Data collection: I.G., F.S., M.S., F.W.A.W., and I.U. Data analysis: I.G., and I.U.; Analysis verification: I.U. Writing: original draft preparation, I.G., S.F., A.F., M.S., F.W.A.W., and I.U. Writing- review and editing, I.G., J.A.S.,B.A.L., and M.F.; Visual, I.G., I.U.; Supervision: I.U. and M.F. Project administration: I.G., M.S., I.U., and M.F. All authors have agreed to the published version of the manuscript.
Doctoral Thesis
This paper is part of the Doctor Thesis of I.G., supervised by I.U. and M.F.
Congress Participation
Parts of this manuscript have presented at the 84th Swiss National Annual Congress for Orthopedic Surgery and Traumatology (swissorthopaedics), 26-28 June 2024, in Ecublens/Lausanne, and at 33rd National Annual Meeeting of Infectious Diseases, 28-30 August 2024, in Bern, Switzerland.
REFERENCES
1.
Benjamin
A Lipsky, Anthony R Berendt, Paul B Cornia, et al. “2012 Infectious Diseases
Society of America clinical practice guideline for the diagnosis and treatment
of diabetic foot infections.” Clin Infect Dis, vol. 54, no. 12, pp.
132-173, 2012. View at: Publisher Site | PubMed
2.
Lawrence
A Lavery, Edgar J G Peters, David G Armstrong, et al. “Risk factors for
developing osteomyelitis in patients with diabetic foot wounds.” Diabetes
Res Clin Pract, vol. 83, no. 3, pp. 347-352, 2009. View at: Publisher
Site
| PubMed
3.
Arend
J Nieuwland, Felix W A Waibel, Andreas Flury, et al. “Initial antibiotic
therapy for postoperative moderate or severe diabetic foot infections: Broad
versus narrow spectrum, empirical versus targeted.” Diabetes Obes Metab, vol. 25, no.
11, pp. 3290-3297, 2023.
View at: Publisher
Site
| PubMed
4.
Nicolas W Cortes-Penfield, David G Armstrong, Meghan B
Brennan, et al. « Evaluation
and Management of Diabetes-related Foot Infections.” Clin Infect Dis,
vol. 77, no. 3, pp. e1-e13, 2023. View at: Publisher Site | PubMed
5.
Javier
Aragón-Sánchez, Benjamin A Lipsky “Modern management of diabetic foot
osteomyelitis. The when, how and why of conservative approaches.” Expert Rev
Anti Infect Ther, vol. 16, no. 1, pp. 35-50, 2018. View at: Publisher
Site
| PubMed
6.
Eric
Senneville, Olivier Robineau “Treatment options for diabetic foot
osteomyelitis.” Expert Opin Pharmacother, vol. 18, no. 8, pp.
759-765, 2017. View at: Publisher
Site
| PubMed
7.
Shiwei
Zhou, Brian M Schmidt, Oryan Henig, et al. “Deferring Amputation in Diabetic
Foot Osteomyelitis: Doing More Harm Than Good?” Open Forum Infect Dis,
vol. 8, no. 7, pp. ofab184, 2021. View at: Publisher Site | PubMed
8.
Ilker
Uçkay, Karim Gariani, Victor Dubois-Ferrière, et al. “Diabetic foot infections:
recent literature and cornerstones of management.” Curr Opin Infect Dis,
vol. 29, no. 2, pp. 145-152, 2016. View at: Publisher
Site
| PubMed
9.
Whitney
Miller, Chrystal Berg, Michael L Wilson, et al. “Risk Factors for
Below-the-Knee Amputation in Diabetic Foot Osteomyelitis After Minor
Amputation.” J Am Podiatr Med Assoc, vol. 109, no. 2, pp. 91-97, 2019.
View at: Publisher
Site
| PubMed
10. Thomas V Häller, Peter Kaiser,
Dominik Kaiser, et al. “Outcome of Ray Resection as Definitive Treatment in
Forefoot Infection or Ischemia: A Cohort Study.” J Foot Ankle
Surg,
vol.59, no. 1, pp. 27-30, 2020. View at: Publisher Site | PubMed
11. Éric
Senneville, Zaina Albalawi, Suzanne A van Asten, et al. “IWGDF/IDSA guidelines on the
diagnosis and treatment of diabetes-related foot infections (IWGDF/IDSA 2023).”
Diabetes Metab Res Rev, vol. 40, no. 3, pp. 3687, 2024. View at: Publisher Site | PubMed
12. Nese Saltoglu, Serkan Surme, Elif
Ezirmik, et al. “KLİMİK Society, Diabetic Foot Study
Group. The Effects of Antimicrobial Resistance and the Compatibility of Initial
Antibiotic Treatment on Clinical Outcomes in Patients With Diabetic Foot
Infection.” Int J Low Extrem Wounds,
vol. 22, no. 2, pp. 283-290, 2023. View at: Publisher
Site
| PubMed
13. Laura Soldevila-Boixader, Oscar
Murillo, Felix W A Waibel, et al. “The Epidemiology of Antibiotic-Related
Adverse Events in the Treatment of Diabetic Foot Infections: A Narrative Review
of the Literature.” Antibiotics (Basel), vol. 12, no. 4, pp. 774, 2023.
View at: Publisher Site | PubMed
14. Felix W A Waibel, Ilker Uçkay, Kati
Sairanen, et al. “Diabetic calcaneal osteomyelitis.” Infez Med, vol. 27,
no. 3, pp. 225-238, 2019. View at: PubMed
15. Tsola Efejuku, Shivan N Chokshi,
Daniel Jupiter, et al. “Retrospective Study Analyzing Risk Factors of Foot and
Ankle Amputation in Patients with Diabetes Diagnosed with Osteomyelitis.” Foot
Ankle Orthop, vol. 7, no. 1, pp. 2473011421S00185, 2022. View at: Publisher
Site
| PubMed
16. Aroa Tardáguila-García, Irene
Sanz-Corbalán, Josep M García-Alamino, et al. “Medical Versus Surgical
Treatment for the Management of Diabetic Foot Osteomyelitis: A Systematic
Review.” J
Clin Med,
vol. 10, no.6, pp. 1237, 2021. View at: Publisher Site | PubMed
17. Elin Winkler,
Madlaina Schöni, Nicola Krähenbühl, et al. “Foot Osteomyelitis Location and Rates of Primary or
Secondary Major Amputations in Patients With Diabetes.” Foot Ankle Int,
vol. 43, no. 7, pp. 957-967, 2022. View at: Publisher
Site
| PubMed
18. Paul Zeun, Catherine Gooday, Ian
Nunney, et al. “Predictors of Outcomes in Diabetic Foot Osteomyelitis Treated
Initially With Conservative (Nonsurgical) Medical Management: A Retrospective
Study.” Int
J Low Extrem Wounds, vol. 15, no. 1, pp. 19-25, 2016. View at: Publisher
Site
| PubMed
19. Flavien Mauler,
Florian Wanivenhaus, Thomas Böni, et al. “Nonsurgical Treatment of Osteomyelitis of the Hallux
Sesamoids: A Case Series and Literature Review.” J Foot Ankle Surg, vol.
56, no. 3, pp. 666-669, 2017. View at: Publisher
Site
| PubMed
20. Javier Aragón-Sánchez, Jose L
Lázaro-Martínez, Francisco Javier Alvaro-Afonso, et al. “Conservative Surgery
of Diabetic Forefoot Osteomyelitis: How Can I Operate on This Patient Without
Amputation?” Int J Low Extrem Wounds, vol. 14, no. 2, pp. 108-131, 2015.
View at: Publisher Site | PubMed
21. Sachin Allahabadi, Kareem B Haroun,
Daniel M Musher, et al. “Consensus on surgical aspects of managing
osteomyelitis in the diabetic foot.” Diabet Foot Ankle, vol. 7, pp.
30079, 2016. View at: Publisher Site | PubMed
22. Ezio Faglia, Giacomo Clerici,
Maurizio Caminiti, et al. “Influence of osteomyelitis location in the foot of
diabetic patients with transtibial amputation.” Foot Ankle Int,
vol. 34, no. 2, pp. 222-227, 2013. View at: Publisher
Site
| PubMed
23. Matthieu Zingg, Alain Lacraz, ,
Helia Robert-Ebadi, et al. “Transcutaneous Oxygen Pressure Values Often Fail to
Predict Stump Failures after Foot or Limb Amputation in Chronically Ischemic
Patients.” Clin Surg, vol. 4, pp. 2366, 2019. View at: Publisher Site
24. Alina Tone, Sophie Nguyen, Fabrice
Devemy, et al. “Six-week versus twelve-week antibiotic therapy for
nonsurgically treated diabetic foot osteomyelitis: a multicenter open-label
controlled randomized study.” Diabetes Care, vol. 38, no. 4, pp.
302-307, 2015. View at: Publisher Site | PubMed
25. Furrer PR, Schöni M, Waibel FWA, et
al. “Lack of Benefit of Routine Serum Laboratory Control Samples during
Treatment of Diabetic Foot Infection.” Arch Microbiol Immunol, vol. 6,
no. 1, pp. 115-122, 2022. View at: Publisher Site
26. Benjamin A Lipsky “Treating diabetic
foot osteomyelitis primarily with surgery or antibiotics: have we answered the
question?” Diabetes Care, vol. 37, no. 3, pp. 593-595, 2014. View at: Publisher Site | PubMed
27. José Luis Lázaro Martínez, Yolanda
García Álvarez, Aroa Tardáguila-García, et al. “Optimal management of diabetic
foot osteomyelitis: challenges and solutions.” Diabetes Metab Syndr Obes,
vol. 12, pp. 947-959, 2019. View at: Publisher Site | PubMed
28. Zulfiqarali G Abbas, Raidah R
Gangji, Ilker Uçkay “Antibiotic Stewardship in the Management of Infected
Diabetic Foot Ulcer Disease in Less Developed Countries.” Endocrinol
Diabetes Metab, vol. 7, no. 4, pp. e00503, 2024. View at: Publisher Site | PubMed
29. Shaima Kmari-El-Ghazouany, Aroa
Tardáguila-García, Mateo López-Moral, et al. “Comparative Analysis of Bone
Resection Versus Bone Curettage in Diabetic Foot Osteomyelitis.” Int J Low
Extrem Wounds, vol. 24, no. 1, pp. 143-148, 2025. View at: Publisher
Site
| PubMed
30. Sameh R Moosa, Ali H Allan, Amr N Younes, et al. “Percutaneous Partial Bone Excision in the Management of Diabetic Toe Osteomyelitis.” Foot Ankle Int, vol. 44, no. 9, pp. 836-844, 2023. View at: Publisher Site | PubMed